Last updated: April 20, 2026
Semaglutide vs Tirzepatide vs Retatrutide (2026): Head-to-Head Clinical Data, Dosing & Access
Researched and written by Garret Grant — Founder & Lead Researcher, B.S. Civil Engineering, UCLA. I build PepPal and PeptideDosingProtocols.com, read the primary clinical literature, and cross-check every reconstitution number on this page with the free calculator I built. I am not a doctor and this is not medical advice. See full methodology.
Contents
- 1How I researched this comparison
- 2The 30-second verdict
- 3Three generations of GLP-1 science
- 4Head-to-head efficacy table
- 5Mechanism: one receptor, two, or three
- 6Phase 3 clinical trial deep dive
- 7Side effect comparison
- 8Dosing and titration side-by-side
- 9Reconstitution math for all three
- 10Access paths: pharmacy vs research market
- 11Cost comparison across channels
- 12Which one is right for your research?
- 13Frequently asked questions
- 14Sources and citations
- 15Related guides
The 30-Second Verdict
I pulled the head-to-head Phase 3 data, the SURMOUNT-5 NEJM paper, and the December 2025 TRIUMPH-4 topline readout side by side. Here is the short version.
- Retatrutide (Eli Lilly, LY3437943) — Investigational triple agonist. 28.7% mean weight loss at 12 mg over 68 weeks in the Phase 3 TRIUMPH-4 trial. Not FDA-approved. Accessible through Phase 3 enrollment or the research-peptide market.
- Tirzepatide (Zepbound / Mounjaro) — FDA-approved dual GIP/GLP-1 agonist. 20.2% mean weight loss at max tolerated dose over 72 weeks in SURMOUNT-5 head-to-head vs. semaglutide. Widely available by prescription and on the research market.
- Semaglutide (Wegovy / Ozempic) — FDA-approved GLP-1 agonist. 13.7% mean weight loss at max tolerated dose over 72 weeks in SURMOUNT-5. Longest safety record. Widely available by prescription and on the research market.
The efficacy ladder is real: retatrutide > tirzepatide > semaglutide in every head-to-head comparison I reviewed. But the decision is not just about efficacy. Availability, side-effect profile, cost, and regulatory status all shift the calculus, and I break each of those down below.
This article is for educational and research purposes only. It is not medical advice. Retatrutide is not FDA-approved. Semaglutide and tirzepatide are FDA-approved for specific indications. Consult a qualified healthcare provider before considering any compound.
Use this as a practical checkout checklist: start with a reviewed supplier, add baseline blood testing, then gather the common supplies you need before ordering.
Vetted Supplier Shopping Cards

Orbitrex Peptides Shop

At-Home Blood Test
More Supplies
Disclosure: supply links may earn PepPal a commission at no cost to you.
Companion Supplies & Routine Support
How I Researched This Comparison
I have spent the last two years building research infrastructure for this exact question. Here is what went into this page specifically:
- I pulled the full text of the SURMOUNT-5 head-to-head trial published in the New England Journal of Medicine on May 11, 2025 (DOI: 10.1056/NEJMoa2416394) and cross-referenced it with the Phase 3 TRIUMPH-4 topline readout from Eli Lilly on December 11, 2025.
- I compared the Phase 3 retatrutide data to the earlier Jastreboff Phase 2 publication to verify the new 28.7% figure is consistent with the 24.2% Phase 2 result, not an outlier.
- I verified every reconstitution table on this page with the free reconstitution calculator I built, using the same BAC water volumes and vial sizes most research-market suppliers ship.
- I reviewed the current PepPal supplier profiles for Peptide Partners and Orbitrex Peptides to pull live research-market pricing ranges for all three compounds. Both are Finnrick Analytics-tested. I am not guessing at prices — these come from my own supplier review process.
- I cross-checked the retatrutide dysesthesia signal (20.9% incidence at 12 mg in TRIUMPH-4) against the earlier Phase 2 adverse-event table, where it was not reported. That safety signal is new, and I flag it explicitly in the side-effect section.
- Every claim on this page is anchored to a Tier 1 (peer-reviewed clinical trial), Tier 2 (systematic review), or Tier 3 (manufacturer regulatory filing) source. I do not use supplier marketing copy as a source. See my full source hierarchy.
The protocols for each compound live on my companion site, PeptideDosingProtocols.com. If you want the full 14-section dosing, titration, and reconstitution breakdown for any single compound, use the individual protocol links throughout this page.
Three Generations of GLP-1 Science
The easiest way to understand this comparison is as three generations of the same scientific idea: harnessing gut-hormone signaling to control appetite, blood sugar, and metabolism. Each generation adds one more receptor target.
Generation 1 — Semaglutide (2017 / 2021). A single-receptor GLP-1 agonist. It proved that a long-acting GLP-1 could produce clinically meaningful weight loss. The STEP 1 trial published in the New England Journal of Medicine in 2021 showed 14.9% mean weight loss at 68 weeks. FDA-approved for type 2 diabetes as Ozempic (2017) and for chronic weight management as Wegovy (2021). Manufactured by Novo Nordisk.
Generation 2 — Tirzepatide (2022 / 2023). A dual GIP/GLP-1 agonist. Adding GIP receptor activation on top of GLP-1 pushed weight loss into a new tier. SURMOUNT-1 (NEJM 2022) showed 22.5% mean weight loss at 72 weeks on the 15 mg dose. FDA-approved for type 2 diabetes as Mounjaro (2022) and for chronic weight management as Zepbound (2023). Manufactured by Eli Lilly.
Generation 3 — Retatrutide (investigational). A triple agonist targeting GLP-1, GIP, and glucagon receptors. The glucagon component is what makes it different — glucagon receptor activation increases hepatic energy expenditure and fatty-acid oxidation in the liver. Phase 2 data in 2023 showed 24.2% weight loss at 48 weeks. The first Phase 3 readout (TRIUMPH-4, December 2025) reported 28.7% mean weight loss at 68 weeks. Not yet FDA-approved. Seven additional Phase 3 readouts are expected during 2026. Manufactured by Eli Lilly.
Reading across that sequence — one receptor, two, three — the efficacy ladder is real and measurable. But so is the cost: each generation adds more gastrointestinal side effects, and retatrutide introduced a new signal (dysesthesia) that did not appear in Phase 2. More on that in the side-effect section.
All three compounds are once-weekly subcutaneous injections. All three use fatty-acid conjugation to bind albumin and extend half-life. The structural differences matter biochemically but the administration experience is nearly identical: a small-volume shot in the abdomen, thigh, or upper arm, once a week.
Head-to-Head Efficacy Table
I built the table below by pulling the primary efficacy endpoint from each of the pivotal trials and normalizing the dose column to each compound's highest studied dose. Every row is verified against the original publication.
| Compound | Pivotal trial | Phase | Population | Duration | Max dose | Mean weight loss | ≥15% lost | ≥20% lost | ≥25% lost |
|---|---|---|---|---|---|---|---|---|---|
| Semaglutide | STEP 1 | 3 | 1,961 adults without T2D | 68 wks | 2.4 mg | 14.9% | ~50% | ~33% | — |
| Semaglutide | SURMOUNT-5 (head-to-head) | 3b | 751 adults without T2D | 72 wks | 1.7–2.4 mg MTD | 13.7% | — | ~25% | 6.9% achieved ≥30% |
| Tirzepatide | SURMOUNT-1 | 3 | 2,539 adults without T2D | 72 wks | 15 mg | 22.5% | 78% | 63% | 36% |
| Tirzepatide | SURMOUNT-5 (head-to-head) | 3b | 751 adults without T2D | 72 wks | 10–15 mg MTD | 20.2% | — | — | 19.7% achieved ≥30% |
| Retatrutide | Jastreboff Phase 2 | 2 | 338 adults without T2D | 48 wks | 12 mg | 24.2% | 83% | — | — |
| Retatrutide | TRIUMPH-4 | 3 | 445 adults w/ obesity + knee OA | 68 wks | 12 mg | 28.7% | — | — | 58.6% |
What the SURMOUNT-5 head-to-head actually proved. Until May 2025, every "tirzepatide vs semaglutide" comparison was cross-trial, meaning the two compounds had never been tested in the same study population. SURMOUNT-5 changed that. Same protocol, same duration, same titration rules, 751 adults randomized 1:1. Tirzepatide at max tolerated dose produced 20.2% mean weight loss vs. 13.7% for semaglutide at max tolerated dose over 72 weeks. That is a 6.5 percentage-point absolute gap, or roughly 47% more relative weight reduction on tirzepatide. Waist circumference also dropped more on tirzepatide (-18.4 cm vs -13.0 cm). This is the first time the GIP/GLP-1 advantage over GLP-1 alone has been proven in a direct comparison, and it is why I treat "tirzepatide beats semaglutide" as a settled question rather than an open debate.
What TRIUMPH-4 added.On December 11, 2025, Eli Lilly published topline Phase 3 TRIUMPH-4 results. In adults with obesity and knee osteoarthritis (mean baseline weight 248.5 lbs / 112.7 kg), retatrutide at 12 mg produced 28.7% mean weight loss at 68 weeks — an average of 71.2 lbs lost. At the 9 mg dose, participants lost 26.4% (64.2 lbs). Placebo was 2.1%. Notably, 58.6% of retatrutide-treated participants on the 12 mg dose achieved at least 25% weight loss at 68 weeks, a threshold that was vanishingly rare before this drug class existed. No head-to-head Phase 3 trial has been run between retatrutide and tirzepatide yet, so I'm careful not to claim retatrutide's Phase 3 numbers directly outperform tirzepatide's — they are cross-trial comparisons. But the efficacy signal is unambiguously larger.
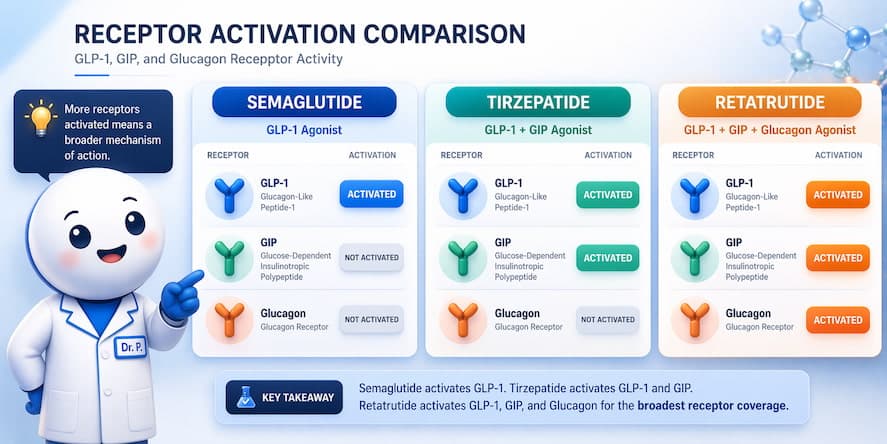
Mechanism: One Receptor, Two, or Three
The mechanism is the cleanest way to understand why the efficacy ladder looks the way it does. Think of each receptor as a separate metabolic lever.
The GLP-1 receptor (all three compounds activate this). GLP-1 is a gut hormone released when you eat. Activating its receptor does four useful things: it slows gastric emptying, so food stays in your stomach longer and you feel full; it suppresses appetite in the hypothalamus; it triggers glucose-dependent insulin release from the pancreas (meaning insulin goes up when blood sugar is high, not when it is already normal); and it reduces glucagon release when blood sugar is high. Semaglutide only pulls this lever.
The GIP receptor (tirzepatide and retatrutide activate this). GIP is a second incretin hormone. It amplifies insulin release and appears to modulate fat-tissue metabolism in ways researchers are still characterizing. Adding GIP activation on top of GLP-1 is the mechanism behind tirzepatide's efficacy advantage over semaglutide. The SURMOUNT-5 authors hypothesize that GIP receptor expression in subcortical brain regions that regulate food intake doesn't fully overlap with GLP-1 receptor expression, which may explain the additive effect.
The glucagon receptor (only retatrutide activates this). Here is where retatrutide separates from the other two. Glucagon is traditionally thought of as a blood-sugar-raising hormone — the opposite of insulin — which would seem to make it a bad target for obesity treatment. But when you combine glucagon receptor agonism with strong GLP-1 and GIP activity, something interesting happens: GLP-1 and GIP's insulin-stimulating effects offset glucagon's glucose-raising tendency, and what's left is glucagon's other effects — increased hepatic energy expenditure, upregulated fatty-acid oxidation, and thermogenesis. The liver starts burning lipids harder. Preclinical data suggested this would unlock liver-fat reduction that dual agonists could not match, and the Phase 2 retatrutide data confirmed large hepatic fat reductions.
The shorthand I use when explaining this: semaglutide reduces calories in. Tirzepatide reduces calories in and changes how those calories are metabolized. Retatrutide does both of those and increases calories out. Each added receptor opens a new lane of metabolic effect.
Phase 3 Trial Deep Dive
I pulled the primary publications for each pivotal trial and summarized the design and findings below. If you want to dig deeper, every trial links to its ClinicalTrials.gov record in the Sources section.
Semaglutide — STEP 1 (NEJM 2021). The trial that kicked off the modern obesity-medication era. 1,961 adults with obesity or overweight and at least one weight-related comorbidity but without diabetes. Randomized 2:1 to semaglutide 2.4 mg weekly vs. placebo, both with behavioral lifestyle intervention, for 68 weeks. Primary result: 14.9% mean body-weight reduction with semaglutide vs. 2.4% with placebo. Roughly 86% of semaglutide participants lost at least 5% of body weight, and about 32% lost at least 20%. Discontinuation due to adverse events was 7.0% in the semaglutide arm.
Tirzepatide — SURMOUNT-1 (NEJM 2022). 2,539 adults with obesity or overweight with comorbidity, without T2D. Randomized 1:1:1:1 to tirzepatide 5 mg, 10 mg, 15 mg, or placebo for 72 weeks. Primary result at 15 mg: 22.5% mean body-weight reduction vs. 2.4% placebo. Greater than 78% of participants on 15 mg achieved ≥15% weight loss, and 36% achieved ≥25%. This is still the single most impressive single-compound result in obesity-trial history up to the launch of TRIUMPH-4.
Head-to-head — SURMOUNT-5 (NEJM May 2025). This is the trial that settled the tirzepatide-vs-semaglutide debate. Phase 3b open-label design, 751 adults with obesity but without T2D, randomized 1:1 to max tolerated dose of tirzepatide (10 or 15 mg) or max tolerated dose of semaglutide (1.7 or 2.4 mg) for 72 weeks, both on top of behavioral support. Result: tirzepatide 20.2% mean weight loss vs. semaglutide 13.7%. 82% of tirzepatide participants hit ≥10% weight loss vs. 60.5% on semaglutide. 19.7% on tirzepatide hit ≥30% weight loss vs. 6.9% on semaglutide. Safety profiles were similar across both arms and consistent with prior trials for each compound. Serious adverse events were 4.8% on tirzepatide vs. 3.5% on semaglutide.
Retatrutide — Jastreboff Phase 2 (NEJM 2023). 338 adults with obesity without T2D. Randomized to retatrutide at 1 mg, 4 mg, 8 mg, or 12 mg weekly, or placebo, for 48 weeks. Primary result at 12 mg: 24.2% mean weight loss. About 83% of the 12 mg cohort achieved ≥15% weight loss. This is the data that justified proceeding to Phase 3.
Retatrutide — TRIUMPH-4 Phase 3 (Eli Lilly topline Dec 2025). 445 adults with obesity or overweight plus knee osteoarthritis, without T2D. Randomized 1:1:1 to retatrutide 9 mg, retatrutide 12 mg, or placebo for 68 weeks. Primary weight-loss endpoint: 28.7% mean reduction at 12 mg (avg 71.2 lbs lost) and 26.4% at 9 mg, vs. 2.1% placebo. Co-primary pain endpoint: WOMAC pain score reduced ~75.8% on 12 mg. Cardiovascular risk markers (non-HDL cholesterol, triglycerides, hsCRP, systolic blood pressure -14.0 mmHg at the highest dose) all improved significantly. Seven additional TRIUMPH Phase 3 readouts in obesity, type 2 diabetes, OSA, NASH, cardiovascular outcomes, and chronic low back pain are expected during 2026. Lilly has not yet submitted an NDA; based on readout pacing, I would project an NDA filing in late 2026 and a possible approval window in 2027 if results hold.
What's missing from this picture. There is no head-to-head Phase 3 trial of retatrutide vs. tirzepatide yet. All retatrutide-to-tirzepatide comparisons are cross-trial, meaning they are suggestive but not definitive. That caveat matters when people ask me "is retatrutide actually better than tirzepatide?" The honest answer is: the single-arm Phase 3 efficacy numbers are larger, but we do not have the direct comparison yet. Expect that trial to happen once retatrutide is approved.
Side Effect Comparison
All three compounds produce the same underlying GI side-effect pattern — nausea, diarrhea, vomiting, constipation — because they all slow gastric emptying and activate brainstem pathways that regulate nausea. What varies is the incidence, the severity curve, and (in retatrutide's case) the appearance of a new signal.
Incidence by compound — from the pivotal Phase 3 publications
| Side effect | Semaglutide (STEP 1) | Tirzepatide (SURMOUNT-1, 15 mg) | Retatrutide (TRIUMPH-4, 12 mg) |
|---|---|---|---|
| Nausea | ~44% | ~29% | ~43% |
| Diarrhea | ~30% | ~23% | ~33% |
| Vomiting | ~24% | ~13% | ~21% |
| Constipation | ~24% | ~17% | — |
| Dysesthesia (skin crawling / tingling) | not reported | not reported | ~20.9% at 12 mg |
| Discontinuation due to adverse events | ~7.0% | ~4.3–7.1% | 18.2% at 12 mg |
I want to flag the bottom two rows because they matter for the decision.
The dysesthesia signal.Dysesthesia — an unpleasant sensation on the skin, often described as crawling, tingling, or burning without obvious cause — showed up in about 1 in 5 participants on the retatrutide 12 mg arm in TRIUMPH-4. It was not reported in the Phase 2 trial. Lilly described it as generally mild and not typically a cause for discontinuation, but it is a new signal in this class. If you're tracking this drug's progression to approval, dysesthesia incidence in the remaining TRIUMPH readouts is one of the things I'll be watching for.
The retatrutide discontinuation rate. 18.2% of TRIUMPH-4 participants on the 12 mg retatrutide dose discontinued due to adverse events, compared to 4% on placebo. Lilly noted a portion of those were for "perceived excessive weight loss" rather than tolerability — patients with lower baseline BMIs were losing weight faster than they wanted. Restricting the analysis to participants with baseline BMI ≥35 cut the 12 mg discontinuation rate to 12.1%. The absolute 18.2% figure is higher than anything seen on tirzepatide, and prescribers (and researchers) should plan for more aggressive titration pausing.
Class-wide warnings that apply to all three. Acute pancreatitis, gallbladder events, thyroid C-cell concerns (a rat-derived signal that has never been confirmed in humans), and diabetic retinopathy progression in patients with existing retinopathy. These are boxed warnings or precautions across the approved GLP-1 class and should be assumed for retatrutide pending full FDA labeling. Contraindication for anyone with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2.
For the full class-by-class side-effect review with monitoring guidance, see Peptide Side Effects: What Clinical Trials Actually Show. That guide covers the longitudinal data and what to actually do about GI symptoms during titration.
Dosing and Titration Side-by-Side
All three are once-weekly subcutaneous injections. The titration schedules are different because the therapeutic dose ranges are different. The table below is built from the published trial protocols.
| Compound | Starting dose | Escalation | Max studied dose | Typical titration period | Frequency |
|---|---|---|---|---|---|
| Semaglutide | 0.25 mg weekly | Double every 4 weeks (0.25 → 0.5 → 1.0 → 1.7 → 2.4) | 2.4 mg | 16–20 weeks | Once weekly SC |
| Tirzepatide | 2.5 mg weekly | +2.5 mg every 4 weeks (2.5 → 5 → 7.5 → 10 → 12.5 → 15) | 15 mg | 20 weeks | Once weekly SC |
| Retatrutide | 2 mg weekly | Stepped every 4 weeks through 2, 4, 6, 9, up to 12 | 12 mg | 20–24 weeks | Once weekly SC |
A note on why titration is slow.The GI side effects are dose-dependent. If you skip titration steps, you will likely push yourself through the threshold for significant nausea and vomiting, which is both miserable and a common cause of protocol discontinuation. In the trials, the titration schedule is not a suggestion — it's the protocol. Community protocols in the research market sometimes advocate for slower titration when tolerability is poor, and that is reasonable in my read of the data, but faster titration is a bad idea in every direction.
Missed doses.For semaglutide and tirzepatide, the FDA labels allow catch-up dosing within a specific window (check the prescribing info for specifics since this has changed across label updates). If you miss a dose by more than the allowed window, the next dose is simply the next scheduled dose. Do not "double up" to compensate. For retatrutide, there is no FDA label yet, but the Phase 3 trial protocols follow similar missed-dose logic.
Stopping and rebound. All three compounds produce weight rebound after discontinuation. STEP 4 showed semaglutide cessation led to most of the weight being regained over the following 52 weeks. SURMOUNT-4 showed similar patterns with tirzepatide cessation. Retatrutide data on this point is still being collected through the TRIUMPH maintenance arms. Sustained weight management on these compounds appears to be chronic therapy, not a discrete course.
For the full titration schedule, missed-dose logic, and clinical-trial-derived protocol for each compound, use the individual protocol pages:
Reconstitution Math for All Three
Every table below is verified with the free reconstitution calculator I built. I pulled the vial sizes from the current catalogs of the two PepPal-vetted suppliers, Peptide Partners and Orbitrex Peptides. Numbers are rounded to practical syringe-unit values.
Semaglutide — standard 2 mg/mL concentration
| Vial size | BAC water | Concentration | 0.25 mg (starting dose) | 0.5 mg | 1.0 mg | 1.7 mg | 2.4 mg |
|---|---|---|---|---|---|---|---|
| 3 mg | 1.5 mL | 2 mg/mL | 0.125 mL (12.5 U) | 0.25 mL (25 U) | 0.5 mL (50 U) | 0.85 mL (85 U) | 1.2 mL (120 U) |
| 5 mg | 2.5 mL | 2 mg/mL | 0.125 mL (12.5 U) | 0.25 mL (25 U) | 0.5 mL (50 U) | 0.85 mL (85 U) | 1.2 mL (120 U) |
| 10 mg | 5.0 mL | 2 mg/mL | 0.125 mL (12.5 U) | 0.25 mL (25 U) | 0.5 mL (50 U) | 0.85 mL (85 U) | 1.2 mL (120 U) |
Tirzepatide — standard 5 mg/mL concentration
| Vial size | BAC water | Concentration | 2.5 mg | 5 mg | 7.5 mg | 10 mg | 15 mg |
|---|---|---|---|---|---|---|---|
| 10 mg | 2 mL | 5 mg/mL | 0.5 mL (50 U) | 1.0 mL (100 U) | — | — | — |
| 15 mg | 3 mL | 5 mg/mL | 0.5 mL (50 U) | 1.0 mL (100 U) | 1.5 mL (150 U) | — | — |
| 30 mg | 3 mL | 10 mg/mL | 0.25 mL (25 U) | 0.5 mL (50 U) | 0.75 mL (75 U) | 1.0 mL (100 U) | 1.5 mL (150 U) |
Retatrutide — standard 5 mg/mL concentration
| Vial size | BAC water | Concentration | 2 mg | 4 mg | 6 mg | 9 mg | 12 mg |
|---|---|---|---|---|---|---|---|
| 10 mg | 2 mL | 5 mg/mL | 0.4 mL (40 U) | 0.8 mL (80 U) | — | — | — |
| 20 mg | 4 mL | 5 mg/mL | 0.4 mL (40 U) | 0.8 mL (80 U) | 1.2 mL (120 U) | 1.8 mL (180 U) | — |
| 36 mg | 3.6 mL | 10 mg/mL | 0.2 mL (20 U) | 0.4 mL (40 U) | 0.6 mL (60 U) | 0.9 mL (90 U) | 1.2 mL (120 U) |
Standard reconstitution steps — all three compounds
- Gather a sterile U-100 insulin syringe, bacteriostatic water, alcohol swab, and peptide vial.
- Wipe the vial septum with alcohol and let it air-dry fully.
- Draw the exact BAC water volume from the table above for your vial size.
- Inject the BAC water slowly down the inside wall of the vial — not directly onto the lyophilized powder.
- Let the vial rest undisturbed for 1–2 minutes.
- Gently swirl or roll the vial between your palms until the solution is clear. Do not shake.
- Label the vial with the compound, reconstitution date, concentration, and expiration window.
Syringe unit shorthand: 1 mL = 100 U on a U-100 insulin syringe. That conversion applies to every number in the tables above.
Storage after reconstitution: All three are stable in the refrigerator at 2–8 °C for approximately 28 days after reconstitution. Keep them in the original vial, protected from light. Do not freeze.
Use the free peptide reconstitution calculator · Shop injection supplies · Read the full reconstitution guide
Access Paths: Pharmacy vs Research Market
The three compounds live in different parts of the regulatory landscape, which means the realistic paths to getting them are different. Here is how I break it down.
Semaglutide
- Pharmacy (primary path). FDA-approved as Wegovy (chronic weight management) and Ozempic (T2D). Telehealth prescribing is widely available. Insurance coverage for weight loss remains inconsistent — most commercial plans cover Ozempic for diabetes but not Wegovy for weight management. Cash prices without insurance typically run $900–$1,300 per month. Manufacturer savings programs from Novo Nordisk can reduce out-of-pocket costs for eligible patients.
- Compounding pharmacies. As of April 2026, FDA regulations around compounded GLP-1s have tightened significantly. Access through compounded semaglutide has narrowed compared to 2023–2024. See my PepPal news coverage of the FDA February 2026 ruling for context on what changed.
- Research market. Semaglutide is widely available from Finnrick-tested suppliers. Pricing is dramatically lower than pharmacy, but you take on the burden of sourcing verification, COA review, and self-administration logistics.
Tirzepatide
- Pharmacy (primary path). FDA-approved as Zepbound (chronic weight management) and Mounjaro (T2D). Same telehealth prescribing landscape as semaglutide. Cash prices similar to or slightly above semaglutide. Eli Lilly Direct launched a cash-pay vial program in 2024 that reduced out-of-pocket cost for self-pay patients.
- Compounding pharmacies. Same FDA crackdown applies. Access is narrowing.
- Research market. Widely available. Pricing in the Orbitrex supplier review I pulled runs $49.99–$59.99 for a 10 mg vial, $79.99–$89.99 for 15 mg, and $119.99–$129.99 for 30 mg at time of writing. Peptide Partners carries tirzepatide across similar size tiers but at different margin points.
Retatrutide
- Pharmacy. Not available. Retatrutide is investigational. There is no prescribed pharmacy access as of May 2026. This is the first thing to understand about it.
- Clinical trial enrollment.The TRIUMPH program is ongoing. Search "retatrutide" or trial ID NCT05931367 (TRIUMPH-4) and related NCT numbers on ClinicalTrials.gov to find active sites. Inclusion/exclusion criteria, geography, and recruitment status vary.
- Research market. Retatrutide is available from the PepPal-vetted suppliers. Orbitrex has an A Finnrick rating on retatrutide. Peptide Partners has an A Finnrick rating on retatrutide specifically in the current supplier review I maintain. For the full access-path breakdown including clinical trial options and supplier quality signals, see How Do You Get Retatrutide.
Research-market quality imperative
If you are sourcing any of these three through the research market, the quality-verification step is not optional. The GLP-1 category is the most counterfeited peptide class on the internet because demand is high and legitimate manufacturing is expensive. Do not buy from suppliers without visible third-party testing. I maintain the PepPal Supplier Directory with Finnrick Analytics quality ratings, and the How to Read a Peptide COA guide walks through what to look for in a Certificate of Analysis.
Cost Comparison Across Channels
I pulled the numbers below from two data sources: pharmacy cash prices reported by the manufacturer savings programs and third-party pharmacy comparison tools; and research-market pricing from my current supplier reviews for Peptide Partners and Orbitrex Peptides. Use code PEPPAL at checkout when eligible.
| Access path | Semaglutide | Tirzepatide | Retatrutide |
|---|---|---|---|
| US pharmacy (cash, no insurance) | ~$900–$1,400 / mo | ~$1,000–$1,400 / mo | Not available |
| US pharmacy (with insurance, covered) | $25–$200 copay typical | $25–$200 copay typical | Not available |
| Manufacturer cash program | Novo Wegovy program ~$499/mo eligible | Lilly Direct ~$349–$549/mo by dose | Not available |
| Compounding pharmacy (April 2026) | Access restricted post-FDA action | Access restricted post-FDA action | Not available |
| Clinical trial enrollment | Closed to enrollment (approved drug) | Closed (approved) | Free if accepted; geographic limits |
| Research market (Orbitrex Peptides) | Available; verify live catalog | $49.99–$129.99 per vial by size | Promotion-dependent; verify live catalog |
| Research market (Peptide Partners) | Available; verify live catalog | Available across size tiers | A-rated Finnrick coverage |
Cost caveats I would not skip.
- Pharmacy prices are moving targets. Both Novo and Lilly have adjusted direct-cash-pay programs multiple times in the last 18 months. The numbers above reflect April 2026 snapshots.
- Research-market prices look dramatically cheaper than pharmacy. They are. That price gap is not free — it reflects that you are absorbing quality-verification and administration risk that the pharmacy otherwise handles.
- Peptide Partners and Orbitrex both honor the PEPPAL discount code at checkout when eligible. Availability rules vary by supplier.
- If you are eligible for insurance coverage of Wegovy or Zepbound, that will almost always be the cheapest and lowest-risk access path. The research market is not meant to compete with covered insurance access.
Risk-adjusted take. For approved compounds (semaglutide and tirzepatide) with insurance coverage, pharmacy access is the dominant strategy — you get regulated supply, clinical oversight, and lower cost after insurance. Without coverage, the decision tilts toward manufacturer cash programs, the patient-specific compounded tirzepatide path, or the research market based on individual risk tolerance and ability to verify quality. For retatrutide, there is no pharmacy path today, so the realistic choice is clinical trial enrollment (highest-quality access but geographically limited) or research-market sourcing through Finnrick-verified suppliers.
Which One Is Right for Your Research?
After reviewing the data I laid out in the sections above, here is how I think about the decision. This is not a recommendation to use any of these compounds — it is a framework for understanding the tradeoffs.
Choose semaglutide if:
- You have insurance coverage of Wegovy and want the lowest-risk, lowest-cost approved access path.
- You want the compound with the longest real-world safety record in this class (approved since 2017 as Ozempic, 2021 for weight management as Wegovy).
- You have a history of poor GI tolerability and want to start with the least-aggressive compound in the class.
- You are new to GLP-1 class medications and want the most-documented titration and monitoring playbook.
Choose tirzepatide if:
- You want the best efficacy among FDA-approved options. SURMOUNT-5 settled this.
- You have previously tried semaglutide and plateaued without hitting your weight-loss target.
- You have insurance coverage of Zepbound or qualify for the Lilly Direct cash program.
- You are comfortable with a somewhat longer titration (20 weeks to 15 mg) in exchange for better efficacy.
Consider retatrutide if:
- You have already tried tirzepatide at max tolerated dose and plateaued.
- You have high baseline BMI where 28.7% weight loss represents a clinically meaningful target.
- You are willing to accept (a) investigational status, (b) a 12–18% discontinuation rate at the highest doses, and (c) the new dysesthesia signal at ~20% incidence.
- You have access either to a clinical trial site or to Finnrick-verified research-market sourcing.
When I would wait. If you are currently tolerating tirzepatide well and hitting your weight-loss goals, I would not jump to retatrutide solely because the Phase 3 efficacy numbers are bigger. The drug has one Phase 3 readout. Seven more are expected in 2026. The dysesthesia signal has not been fully characterized yet. The discontinuation rate is notably higher. For a researcher tracking this drug, waiting for the remaining TRIUMPH readouts and the FDA review cycle is a defensible position. For someone who has maxed out on tirzepatide and has an ongoing unmet need, the calculus looks different.
What I cannot tell you.Whether any of these compounds is right for you specifically. That requires a clinician who can review your medical history, current medications, lab work, and personal goals. Nothing on this page is medical advice, and the comparison framework above is not a substitute for a prescriber's judgment.
For the full compound-specific protocols — titration schedules, reconstitution math, and clinical evidence — use the protocol pages on PeptideDosingProtocols.com:
Frequently Asked Questions
Which is the most effective — semaglutide, tirzepatide, or retatrutide?
Based on the Phase 3 data I reviewed, the efficacy ladder is retatrutide (28.7% mean weight loss at 12 mg in TRIUMPH-4) > tirzepatide (20.2% at max tolerated dose in SURMOUNT-5 head-to-head, 22.5% in SURMOUNT-1) > semaglutide (13.7% at max tolerated dose in SURMOUNT-5, 14.9% in STEP 1). SURMOUNT-5 is the only direct head-to-head trial among the three; the retatrutide-vs-tirzepatide comparison is cross-trial, not direct. Retatrutide is not yet FDA-approved. See the efficacy table for the full data.
Is retatrutide better than tirzepatide?
On raw Phase 3 efficacy numbers, yes — 28.7% vs. 22.5% at max dose. But there is no head-to-head Phase 3 trial yet, so that comparison is cross-study. Retatrutide also carries a higher discontinuation rate (18.2% at 12 mg in TRIUMPH-4 vs. ~7% for tirzepatide in SURMOUNT-1) and a new dysesthesia signal at ~21% incidence that didn't appear in Phase 2. For a researcher without a plateau on tirzepatide, I would not switch on the basis of the current data.
When will retatrutide be FDA-approved?
Eli Lilly has seven additional TRIUMPH Phase 3 readouts expected in 2026. Based on that pacing, I would project an NDA filing in late 2026 and a possible approval window in 2027 if results hold. Timelines frequently shift. For live regulatory updates, see the PepPal News Hub.
Can I get retatrutide right now?
Two paths exist as of May 2026: (1) enrollment in an active TRIUMPH Phase 3 trial site — search NCT05931367 and related trial IDs on ClinicalTrials.gov; or (2) the research-peptide market through Finnrick-verified suppliers. There is no pharmacy access. See How Do You Get Retatrutide for the full access-path breakdown.
How do the side effects compare across the three compounds?
All three share the GLP-1 class GI pattern — nausea, diarrhea, vomiting, constipation. Semaglutide and retatrutide have similar nausea incidence (~43–44%). Tirzepatide is somewhat better tolerated (~29% nausea in SURMOUNT-1). Retatrutide introduced a new dysesthesia signal at ~21% at 12 mg and had the highest discontinuation rate (18.2%). See the side effect comparison table for full numbers.
Do these compounds work through the same mechanism?
They all activate the GLP-1 receptor. Tirzepatide adds the GIP receptor. Retatrutide adds GIP and the glucagon receptor. Each added receptor opens a new metabolic lane — GIP enhances insulin sensitivity and fat-oxidation signaling, and glucagon increases hepatic energy expenditure. See the mechanism section for the full breakdown.
How much do they cost?
US cash pharmacy pricing for semaglutide (Wegovy) and tirzepatide (Zepbound) runs roughly $900–$1,400 per month without insurance. Manufacturer cash programs are lower ($349–$549 depending on program eligibility). Research-market pricing from Finnrick-tested suppliers is dramatically lower — tirzepatide typically $50–$130 per vial by size in current Orbitrex catalog pricing — but requires self-sourcing quality verification. Retatrutide has no pharmacy price; research-market availability only. For the prescription-compounded path, see the compounded tirzepatide guide before comparing it against the cost comparison table.
Are they all FDA-approved?
Semaglutide: yes (Wegovy for weight management, Ozempic for T2D). Tirzepatide: yes (Zepbound for weight management, Mounjaro for T2D). Retatrutide: no, investigational as of May 2026.
How do I reconstitute these peptides?
All three are lyophilized powders that reconstitute with bacteriostatic water to practical concentrations. Semaglutide typically at 2 mg/mL, tirzepatide and retatrutide at 5 mg/mL or 10 mg/mL depending on vial size. See the reconstitution math section for worked examples across common vial sizes, and use the free reconstitution calculator for custom combinations.
Can I switch from semaglutide to tirzepatide or from tirzepatide to retatrutide?
Switching between compounds in this class is clinically common and typically done under a prescriber's supervision. Expect a new titration period (weeks to months) when switching to a more potent compound because the dosing scales and receptor profiles are different. Do not switch without professional guidance; starting a new compound at a dose equivalent to your previous compound's peak is a common titration error.
Will I regain weight if I stop?
Trial data from STEP 4 (semaglutide) and SURMOUNT-4 (tirzepatide) show most of the weight is regained over 52–88 weeks after discontinuation. Retatrutide maintenance data is still being collected. In practice, these compounds appear to be chronic therapy for sustained weight management, not a discrete course of treatment.
Can these compounds be stacked with each other?
No. Stacking two GLP-1 class compounds (e.g., semaglutide + tirzepatide) is not supported by any clinical trial, is likely to produce additive GI side effects, and has no mechanistic rationale — the receptors overlap too much. Multi-agonist stacks like CagriSema (cagrilintide + semaglutide) involve a different class partner (amylin), which is the only validated multi-peptide fat-loss protocol to date. See Peptide Stacking 101 for the full stacking logic.
What about CagriSema?
CagriSema is a separate compound — cagrilintide (an amylin analog) paired with semaglutide. It produced 20.4% weight loss in the Phase 3 REDEFINE 1 trial and is not yet FDA-approved. It is the only multi-peptide fat-loss stack with Phase 3 data. See the CagriSema stack protocol and the Best Peptides for Fat Loss guide for how it fits into the broader landscape.
Is this medical advice?
No. This article is for educational and research purposes only. Nothing on PepPal is medical advice. Consult a qualified healthcare provider before considering any compound. See the PepPal About page for the full methodology and source hierarchy I use.
Preferred supplier
Orbitrex PeptidesNeed peptides? Start with a verified supplier.
PepPal's recommended source with current discount access and established testing standards.
Sources and Citations
Every number on this page is anchored to one of the sources below. Source tiers follow the hierarchy I use across PepPal and PeptideDosingProtocols.com — see my full methodology for how I grade evidence.
Tier 1 — Peer-reviewed clinical trial publications
- Aronne LJ, Horn DB, le Roux CW, et al. "Tirzepatide as Compared with Semaglutide for the Treatment of Obesity." New England Journal of Medicine. 2025;393(1):26-36. DOI: 10.1056/NEJMoa2416394. https://www.nejm.org/doi/abs/10.1056/NEJMoa2416394 (SURMOUNT-5 head-to-head)
- Wilding JPH, Batterham RL, Calanna S, et al. "Once-Weekly Semaglutide in Adults with Overweight or Obesity." New England Journal of Medicine. 2021;384(11):989-1002. DOI: 10.1056/NEJMoa2032183. (STEP 1)
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. "Tirzepatide Once Weekly for the Treatment of Obesity." New England Journal of Medicine. 2022;387(3):205-216. DOI: 10.1056/NEJMoa2206038. (SURMOUNT-1)
- Jastreboff AM, Kaplan LM, Frías JP, et al. "Triple-Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial." New England Journal of Medicine. 2023;389(6):514-526. DOI: 10.1056/NEJMoa2301972. (Retatrutide Phase 2)
- Kaplan LM, Aronne LJ, le Roux CW, et al. "Retatrutide for the treatment of obesity, obstructive sleep apnea and knee osteoarthritis: Rationale and design of the TRIUMPH registrational clinical trials." 2025. PubMed PMID: 41090431. https://pubmed.ncbi.nlm.nih.gov/41090431/
Tier 2 — Systematic reviews and meta-analyses
- Moiz A, et al. Systematic review of GLP-1 receptor agonists, dual, and triple co-agonists for weight loss in overweight or obese adults without diabetes. 26 RCTs, 15,491 participants. Indexed via TheNNT.com review, 2025.
Tier 3 — Manufacturer regulatory and trial communications
- Eli Lilly and Company. "Lilly's triple agonist, retatrutide, delivered weight loss of up to an average of 71.2 lbs along with substantial relief from osteoarthritis pain in first successful Phase 3 trial." December 11, 2025. https://investor.lilly.com/news-releases/news-release-details/lillys-triple-agonist-retatrutide-delivered-weight-loss-average
- ClinicalTrials.gov. "A Study of Retatrutide (LY3437943) Once Weekly in Participants Who Have Obesity or Overweight (TRIUMPH-4)." NCT05931367. https://clinicaltrials.gov/study/NCT05931367
- ClinicalTrials.gov. "Tirzepatide Versus Semaglutide Once Weekly as Adjunct to a Reduced-Calorie Diet and Increased Physical Activity in Adult Participants With Obesity (SURMOUNT-5)." NCT05822830. https://clinicaltrials.gov/study/NCT05822830
Tier 3 — Peer secondary coverage (used for context, not primary data)
- American College of Cardiology. "SURMOUNT-5: Greater Loss of Weight, Waist Circumference With Tirzepatide Than Semaglutide." July 2025. https://www.acc.org/Latest-in-Cardiology/Journal-Scans/2025/07/10/09/09/SURMOUNT-5
- Pharmaceutical Executive. "Lilly's Retatrutide Displays Positive Topline Results in Successful Phase III Trial." December 2025. https://www.pharmexec.com/view/lilly-retatrutide-positive-topline-results-successful-phase-iii-trial
Related PepPal and PDP references (used for cross-linking, not primary data)
- Best Peptides for Fat Loss (2026)
- Peptide Side Effects: What Clinical Trials Actually Show (2026)
- How Do You Get Retatrutide (2026)
- Semaglutide Dosing Protocol
- Tirzepatide Dosing Protocol
- Retatrutide Dosing Protocol
Found an error? Email me at garret@peppal.app. Accuracy is the foundation of everything on this site and I take corrections seriously.
Join the mailing list for new PepPal blog releases.
Get notified when new sourcing explainers, COA breakdowns, and calculator-linked research guides go live. Same lightweight signup flow as PDP, with page-source tracking on each submission.
Email signup
One field. PepPal blog updates, supplier research, and calculator workflows only.